
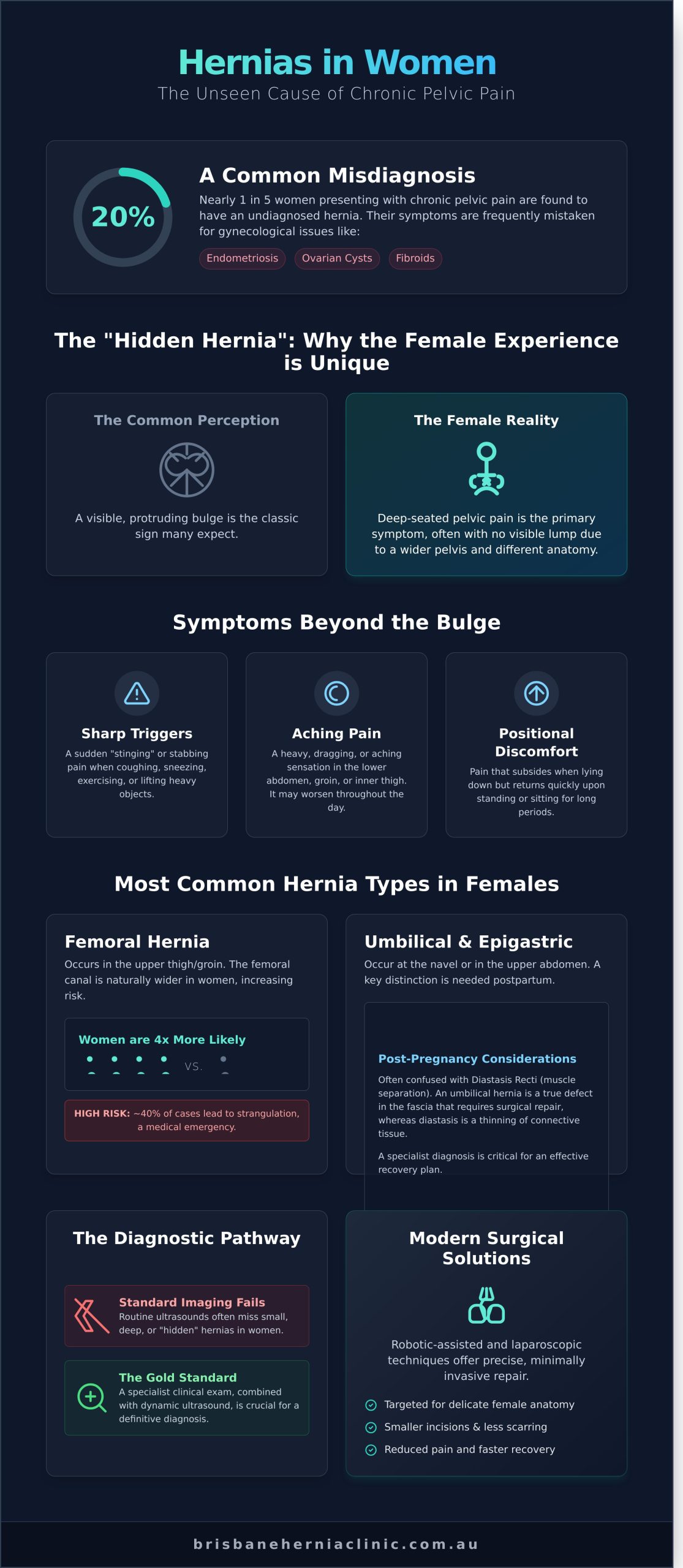
Did you know that nearly 20% of women presenting with chronic pelvic pain are actually suffering from a hernia that was initially misidentified? It’s a frustrating reality when your physical discomfort is dismissed as a gynecological issue or confused with postpartum diastasis recti. You know your body, and you deserve a diagnosis that respects your experience while addressing the root cause of your pain.
In this guide, we detail the specific types of hernias in females that often require a specialist’s eye, from femoral to obturator hernias. You’ll learn how modern Brisbane specialists utilize robotic and laparoscopic technology in 2026 to offer targeted, minimally invasive solutions that prioritize a fast recovery. We’ll walk you through the diagnostic process and our rapid assessment pathway to ensure you move from uncertainty to a pain-free life with confidence.
Key Takeaways
- Understand why many women are frequently misdiagnosed with endometriosis or ovarian cysts and how to identify the true structural source of your pelvic discomfort.
- Explore the specific types of hernias in females, including why femoral and umbilical hernias are significantly more prevalent during and after pregnancy.
- Learn why standard ultrasound imaging often misses small hernias and the importance of a specialist clinical exam for achieving a definitive diagnosis.
- Discover the critical differences between Diastasis Recti and an umbilical hernia to ensure you receive the most effective postpartum care and recovery plan.
- Gain insights into how modern robotic-assisted and minimally invasive techniques provide precise, targeted solutions designed for the delicate female anatomy.
Understanding Hernias in Women: Why the Female Experience is Unique
When you think of a hernia, you likely imagine a visible, protruding bulge. For many women, this simply isn’t the reality. To truly understand What is a hernia?, you must view it as a structural defect in the abdominal wall fascia rather than a simple lump. In our Brisbane practice, we’ve observed that the different types of hernias in females often present as deep-seated pelvic pain. This internal nature frequently leads to misdiagnosis. A 2018 clinical study indicated that approximately 15% of women seeking treatment for chronic pelvic pain were actually suffering from undiagnosed hernias. Instead of receiving hernia repair, these patients are often mismanaged for endometriosis, ovarian cysts, or fibroids for years.
The concept of the “Hidden Hernia” is central to the female experience. Because women generally have a broader pelvis and different fat distribution than men, the defect often sits deeper within the pelvic floor or behind layers of muscle. You won’t always see a bulge, but you will certainly feel the structural compromise. This anatomical “hiding” makes specialized imaging and a high index of clinical suspicion vital for an accurate diagnosis. We focus on identifying these defects early to prevent the progression of symptoms and the risk of tissue strangulation.
The Anatomical Difference: Inguinal Canals in Women
The male inguinal canal is a well-known site for hernias because it’s significantly wider to accommodate the spermatic cord. In women, this canal is much narrower. It houses the round ligament, which provides structural support to the uterus. Because this passageway is tighter, the types of hernias in females that occur here are often smaller in diameter. However, size doesn’t correlate with comfort. These smaller defects frequently cause more intense, localized pain because the abdominal contents are being squeezed through a much smaller opening. This creates a high-pressure environment that irritates surrounding nerves, leading to sharp, debilitating sensations that don’t always align with the “dull ache” described in traditional medical textbooks.
Symptoms That Don’t Include a Bulge
If you don’t have a visible lump, your symptoms might feel frustratingly vague. You might experience a sharp, stabbing pain when you cough, sneeze, or lift a heavy bag of groceries. Many women report an aching sensation that radiates into the labia or inner thigh, often worsening as the day progresses. It’s common for this discomfort to intensify during your menstrual cycle. Hormonal fluctuations can cause mild tissue swelling, which puts additional pressure on the hernia site. This cyclical pattern often leads doctors to incorrectly assume the issue is purely gynecological.
- Aching pain: Often felt as a heavy or dragging sensation in the lower abdomen.
- Sharp triggers: Sudden movements or exercise can cause a “stinging” sensation.
- Positional discomfort: Pain that resolves when lying down but returns quickly upon standing.
Living with an “invisible” physical defect takes a significant psychological toll. When your scans come back clear but your pain persists, it’s easy to feel dismissed by the medical community. At the Brisbane Hernia Clinic, we recognise that your pain is a clinical indicator of a physical problem. We use targeted physical examinations and dynamic ultrasound to find what standard tests often miss. Our goal is to provide a clear diagnosis and a path toward a rapid return to your normal, active lifestyle.
The Most Common Types of Hernias in Females
While inguinal hernias are the most frequent diagnosis globally, the anatomical structure of the female pelvis creates specific vulnerabilities. Understanding the different types of hernias in females is the first step toward effective treatment. Women often experience different symptoms than men, frequently describing a deep, dull ache rather than a visible protrusion.
Femoral Hernias: A Specifically Female Risk
Femoral hernias occur just below the groin crease, where the femoral artery and vein pass into the thigh. This area, known as the femoral canal, is naturally wider in women to accommodate the broader female pelvis. Because of this anatomical difference, women are roughly 4 times more likely than men to develop this specific type. According to healthdirect, certain hernias more common in women like the femoral type require swift medical evaluation. These hernias carry a significantly higher risk of strangulation, occurring in approximately 40% of cases, because the canal is narrow and rigid. You might notice a small lump or persistent pain in the upper thigh or inner groin that intensifies when you lift heavy objects or strain.
Umbilical and Epigastric Hernias
Pregnancy is a primary driver for umbilical hernias in women. As the fetus grows, the abdominal wall stretches and thins, particularly at the linea alba, the midline of the abdomen. Roughly 1 in 10 women may develop a bulge at the navel following multiple pregnancies or a difficult labour. An epigastric hernia occurs slightly higher up, between the belly button and the breastbone. This is often a “fatty” hernia where intra-abdominal fat pushes through a weakened spot in the midline. If you’ve noticed a ‘post-baby’ bulge that doesn’t resolve with core exercises or physical therapy, it’s often a sign of a structural defect rather than simple muscle separation. If the bulge becomes tender or doesn’t flatten when you lie down, you should consult a specialist to discuss your options.
Inguinal and Incisional Hernias
Inguinal hernias occur in the groin and remain the most common of all types of hernias in females, despite being more prevalent in men. In women, these hernias often involve the round ligament, which supports the uterus. The presentation is frequently “occult,” meaning the hernia is hidden behind muscle layers and doesn’t produce a visible lump, making diagnosis via ultrasound or MRI essential.
Incisional hernias are another significant concern, particularly following abdominal surgeries. With C-sections accounting for approximately 36% of births in Australia, the risk of a hernia developing at the scar site is a reality for many. Between 2% and 5% of women who undergo abdominal surgery will develop an incisional hernia within the first two years. These occur because the surgical site remains a permanent point of weakness in the abdominal wall.
Obturator and Pelvic Floor Hernias
Obturator hernias are rare and typically affect older women who have experienced significant weight loss. These hernias protrude through the obturator canal in the pelvic bone. Because they are deep within the pelvis, they rarely cause a visible bulge, making them notoriously difficult to diagnose without advanced imaging. An obturator hernia is a ‘hidden’ cause of inner thigh pain that often mimics nerve compression or hip issues. Similarly, pelvic floor hernias can occur after pelvic organ prolapse or chronic straining, leading to discomfort that feels like a heavy pressure deep within the pelvis. Diagnosis requires a steady hand and an expert mind to differentiate these from more common gynaecological conditions.
Pregnancy, Childbirth, and Postpartum Hernia Risks
Pregnancy represents one of the most significant physiological stressors the female abdominal wall will ever encounter. During the third trimester, your intra-abdominal pressure can increase by up to 200% compared to pre-pregnancy states. This relentless internal force pushes against the abdominal muscles and the linea alba, the connective tissue running down the centre of your stomach. At the same time, your body releases relaxin, a hormone that peaks during the first trimester and remains elevated until birth. Relaxin effectively softens ligaments and connective tissues to facilitate delivery, but it also reduces the structural integrity of the abdominal fascia. This combination of high pressure and softened tissue creates a perfect environment for various types of hernias in females to develop, particularly around the navel or at the site of a previous Caesarean section.
Deciding when to seek surgical intervention is a common concern for Brisbane mothers. If your hernia is small and causes minimal discomfort, we typically recommend delaying surgery until 6 to 12 months after your final pregnancy. Clinical data suggests that repairing a hernia between pregnancies carries a recurrence risk as high as 50% because the subsequent expansion of the abdomen can pull apart the surgical repair. However, if you experience sharp pain, redness, or a bulge that won’t flatten when you lie down, immediate specialist consultation is vital. Understanding the different types of hernias in women helps you identify when a bulge is a minor postpartum change and when it represents a surgical necessity that could lead to bowel obstruction.
The Diastasis Recti Connection
Diastasis recti involves the separation of the rectus abdominis muscles by more than 2.7 cm. While it creates a visible ridge or bulge, it is not a true hernia because the fascial layer remains intact, albeit stretched. However, a true fascial hole or umbilical hernia co-exists in roughly 40% of women with significant muscle separation. While targeted physiotherapy can improve mild cases, a true hernia requires surgical mesh or primary repair to prevent tissue entrapment. At the Brisbane Hernia Clinic, we often assess whether a combined repair is necessary to restore both the strength and the appearance of your abdominal wall.
Postpartum Recovery and Hernia Prevention
The first 12 weeks postpartum are a high-risk period for abdominal strain. Lifting a 4 kg newborn alongside heavy prams can spike internal pressure and worsen existing defects. You should use the “exhale on exertion” breathing technique to lower intra-abdominal spikes by approximately 30%. Engaging a pelvic floor physiotherapist can significantly support your surgical outcomes by stabilizing the deep core muscles. If a “pooch” or bulge remains visible 8 weeks after birth or causes persistent aching during daily activities, it is time for a specialist evaluation to rule out a hernia.
The Diagnostic Pathway: From Chronic Pain to a Clear Answer
Identifying the specific types of hernias in females requires a systematic approach that moves beyond basic screening. Because female anatomy often hides these defects deep within pelvic tissue, a standard physical exam by a general practitioner might not reveal the source of your discomfort. Your journey to recovery begins with a clinical assessment by a hernia specialist. These experts use tactile techniques specifically designed to detect subtle weaknesses in the abdominal wall that are unique to women.
This journey often benefits from a comprehensive, whole-person view of health. An integrative primary care clinic like Holistic Family Practice can be crucial in the early stages of diagnosis, helping to ensure all potential causes of pain are considered before focusing on a specific structural issue.
Specialists focus on the “occult” or hidden nature of these conditions. While a visible bulge is common in men, many women experience “hernia incognita,” where the defect is too small to see but large enough to cause debilitating nerve pain. A specialist’s clinical exam provides the foundation for your diagnosis, but advanced imaging acts as the definitive map for surgical planning.
Why Your Ultrasound Might Be ‘Normal’
A common point of frustration for many patients is receiving a “normal” result from a dynamic ultrasound despite ongoing pain. Statistics from clinical studies indicate that ultrasound can miss up to 25% of small female hernias because the procedure is highly operator-dependent. If the technician doesn’t capture the exact moment of intra-abdominal pressure, the hernia sac may retract, appearing invisible on the screen.
MRI is the gold standard for diagnosing chronic female pelvic pain and identifying small defects. It provides high-resolution, multi-planar views of the pelvic floor and inguinal canal, allowing surgeons to see the relationship between the hernia and surrounding nerves. A negative ultrasound does not rule out a symptomatic hernia. If your symptoms persist, an MRI or a high-resolution CT scan is the necessary next step to find the answer.
Brisbane Specialist Access
Accessing expert care in Queensland requires a structured approach through the Australian healthcare system. You must first visit your Brisbane GP to obtain a formal referral. This document is essential for claiming your Medicare rebate, which in 2026 covers a portion of the specialist consultation fee. For patients with private health insurance, your policy typically covers the costs of diagnostic imaging and hospital fees, though you should verify your specific level of “General Surgery” cover.
The Brisbane Hernia Clinic utilizes a ‘Rapid Access’ pathway to reduce waiting times for symptomatic patients. We understand that living with undiagnosed pain affects your quality of life, so we prioritise diagnostic clarity. Our team coordinates directly with local Brisbane imaging centres that specialise in hernia-specific protocols. This ensures that your scans are read by radiologists who understand the nuances of various types of hernias in females.
If you are tired of living with unexplained pelvic or groin pain, book a consultation with our specialist team to begin your diagnostic pathway today.
Modern Surgical Solutions: Robotic and Minimally Invasive Repair
Alongside surgical advancements, a holistic approach to hernia repair also involves managing contributing risk factors. Reducing excess body weight, for example, can lower the intra-abdominal pressure that strains the abdominal wall, potentially improving long-term surgical outcomes. For individuals looking into comprehensive health strategies, it can be beneficial to explore Semaglutide Weight Loss Program to see how medical weight management can be part of the solution.
Surgical techniques for abdominal wall reconstruction have transformed over the last 20 years. Historically, repairing the various types of hernias in females required large “open” incisions, often measuring 5 to 10 centimeters, which necessitated cutting through healthy muscle and fascia. At Brisbane Hernia Clinic, Dr. McGregor and Dr. Watson prioritise minimally invasive approaches. We utilise advanced laparoscopic and robotic-assisted technology to treat femoral, inguinal, and umbilical defects with millimeter precision. This evolution ensures less tissue trauma, reduced scarring, and a more aesthetic result for our patients.
Robotic-assisted surgery is particularly effective for the female anatomy because it allows for superior visualization of the pelvic floor. The technology provides a 3D, high-definition view that magnifies the surgical field up to 10 times. This clarity is essential when navigating the delicate structures near the round ligament or femoral canal. By using instruments with 360-degree wrist rotation, our surgeons can secure mesh and close defects in tight spaces that are difficult to reach with traditional straight-laparoscopic tools.
The Benefits of Robotic Hernia Repair
Precision is the primary advantage of the robotic platform. When addressing complex types of hernias in females, such as recurrent or multi-defect incisional hernias, the robot allows for a “tension-free” repair. This method significantly lowers the risk of the hernia returning, with recurrence rates in specialist clinics often falling below 2%. Patients benefit from:
- Increased dexterity for repairing small, deep pelvic defects that traditional surgery might miss.
- Significantly reduced post-operative pain, often decreasing the need for strong analgesics by 40% compared to open surgery.
- A faster return to daily Brisbane life, as the tiny 8mm incisions heal much quicker than long surgical wounds.
Recovery and Returning to Activity
The recovery timeline is a major consideration for our active patients. Following a laparoscopic or robotic procedure, approximately 90% of women return home on the same day or within 24 hours. You’ll be encouraged to start light walking immediately to promote circulation. We implement a “Rapid Return” protocol designed to get you back to your routine without compromising the repair. Most patients return to desk-based work within 5 to 7 days. While traditional surgery often sidelined patients for 6 weeks, our minimally invasive techniques typically allow a return to low-impact exercise by day 14 and full gym activities by week 4.
Next Steps: Booking Your Assessment
Your journey to a pain-free life begins with a comprehensive clinical evaluation. During your consultation at our Albany Creek or Taringa locations, we’ll review your symptoms and perform a physical examination. To ensure a productive first appointment, please bring any ultrasound or CT scan results performed within the last 12 months. We also require a detailed list of your current medications and your previous surgical history. Dr. McGregor or Dr. Watson will explain the specific mechanics of your hernia and provide a clear, step-by-step roadmap for your treatment and recovery.
Book your specialist consultation at Brisbane Hernia Clinic today to discuss your options with our expert team. We’re committed to providing the highest standard of care for women across Queensland, ensuring you return to your peak physical health with confidence and safety.
Empowering Your Path to Recovery in 2026
Navigating the various types of hernias in females requires a specialist’s eye, as symptoms often present differently than they do in men. Chronic pelvic pain or a subtle bulge shouldn’t be ignored, especially when the physical demands of pregnancy or postpartum recovery are involved. At the Brisbane Hernia Clinic, we prioritize a diagnostic pathway that moves you from uncertainty to a clear, actionable plan. Led by Dr. Hugh McGregor and Dr. Lindsay Watson, our surgical team specializes in advanced robotic and minimally invasive techniques designed to minimize discomfort and accelerate your healing time.
We’ve streamlined our 2026 patient care model to include Rapid Access Pathways for urgent assessments, ensuring your concerns are addressed with the priority they deserve. You don’t have to live with the persistent ache or the limitation of physical activity that a hernia causes. Our focus remains on restoring your quality of life through precision medicine and compassionate, expert care tailored to the female experience. Take the first step toward a pain-free life, contact our Brisbane specialists today. You’re in safe, experienced hands as you move toward a full and active recovery.
Frequently Asked Questions
Can a female hernia cause pain without a visible lump?
Yes, it’s common for women to experience significant pain from a hernia without any visible bulge. These are often called occult hernias, where the defect in the abdominal wall is too small or deep to be felt during a physical exam. Data suggests that up to 20% of women with chronic pelvic pain actually have a hidden hernia. We use high-resolution ultrasound or MRI at our Brisbane clinic to identify these internal tears that cause deep, aching discomfort.
Is a femoral hernia more dangerous than an inguinal hernia in women?
Yes, femoral hernias carry a much higher risk of complications than the more common inguinal variety. While they only represent about 3% of all hernias, nearly 40% of femoral hernias lead to emergency surgery due to strangulation or incarceration. Because the femoral canal is narrow and rigid, trapped fat or bowel can lose its blood supply within hours. We treat these cases with clinical priority to prevent permanent tissue damage and ensure a safe recovery.
How do I know if my pelvic pain is a hernia or a gynecological issue?
Distinguishing between different types of hernias in females and gynecological conditions like endometriosis requires a methodical diagnostic approach. Hernia pain typically sharpens when you increase intra-abdominal pressure through coughing, lifting, or straining. In contrast, gynecological pain often follows a monthly cycle or feels like a deep, dull pressure. Approximately 15% of our female patients find that their symptoms involve both muscular and reproductive factors, necessitating a collaborative specialist review.
Will a hernia during pregnancy go away on its own after birth?
No, a hernia won’t resolve spontaneously after you give birth because the physical hole in the muscle wall remains. While the pressure on the defect decreases postpartum, the structural weakness persists and may even worsen with subsequent pregnancies. Statistics indicate that 95% of umbilical hernias that appear during pregnancy will eventually require surgical intervention if they become symptomatic. We generally advise waiting 6 to 12 months after delivery before scheduling a permanent robotic or laparoscopic repair.
What is the recovery time for robotic hernia surgery in women?
Most women return to light daily activities within 48 to 72 hours after a robotic-assisted hernia repair. This modern, minimally invasive technique uses tiny 8mm incisions, which significantly lowers the impact on your body compared to traditional open surgery. You’ll typically be able to drive after 5 days and return to full gym activities within 3 to 4 weeks. Our records show that 90% of patients stop taking prescription pain relief by their fourth day of recovery.
Does Medicare cover the cost of female hernia repair in Brisbane?
Yes, Medicare provides rebates for hernia surgery when it’s performed by a specialist surgeon for medical necessity. Under the Medicare Benefits Schedule, items such as 30609 or 30614 cover a portion of the professional fees for the surgeon and anaesthetist. If you have private health insurance, your policy usually covers the hospital theatre and accommodation costs. In Brisbane, Medicare typically contributes between A$450 and A$650 toward the surgical fee, depending on the complexity of the repair.
Can I have a hernia repair if I plan on having more children in the future?
Yes, you can have a hernia repaired before future pregnancies, but the surgical technique must be tailored to your plans. We use specific mesh placement strategies or occasionally non-mesh repairs to ensure the abdominal wall can still expand as your baby grows. While a well-performed repair is durable, there’s a 7% higher risk of the hernia returning after a subsequent pregnancy compared to patients who have finished having children. We’ll discuss these odds during your consultation.
What happens if a female hernia is left untreated?
Leaving a hernia untreated usually leads to the defect enlarging over time, which makes the eventual repair more complex. The primary risk is that a loop of bowel or fatty tissue becomes trapped, a condition that affects roughly 1 in 10 untreated patients. This can lead to a bowel obstruction or strangulation, requiring an emergency operation with a longer recovery path. Understanding the specific types of hernias in females allows us to monitor your condition and perform a planned, minimally invasive procedure before complications arise.